MASTOIDITIS


|
Mastoiditis is a bacterial infection that affects the mastoid portion of the temporal bone and typically presents itself as a red welt behind the pinna. More common in children, it’s characterized by swelling, tenderness, headaches, fever, discharge, and hearing loss in the affected ear. Mastoiditis is commonly accompanied by conductive hearing loss—as seen on the audiogram—due to persistent inflammation of the middle ear and the obstructed transmission of sound. Due to the mastoid air cell system’s honeycomb-like structure, the cells can become infected, often following a recurrent infection in the middle ear. Not only this, but other problems such as a cholesteatoma—a collection of skin cells deep in the ear that prevent proper draining—can lead to an infection such as mastoiditis (Sahi). Once the patient presents their symptoms, a clinician may begin by checking the inside of the ear with an otoscope, which is a lighted tool with a magnifying glass. If mastoiditis is expected, the patient will be referred to an ENT where further tests, like blood and ear cultures, can be performed. Some children may even require a CT scan in order to get a more detailed view of the inside of the skull and the extent of bone involvement. Mastoiditis should be treated as quickly as possible with antibiotics, and in some more serious cases, surgery may be necessary to either drain the middle ear (myringotomy) or remove the inflamed portion of the bone (mastoidectomy). The patient should also do their best to keep the ear as dry as possible to prevent further infection. Although the prognosis for mastoiditis is generally excellent with proper care, treatment is not always easy and the infection may return or even worsen, causing life-threatening issues such as blood clots and meningitis (Mastoiditis). |
PAGET'S DISEASE
|
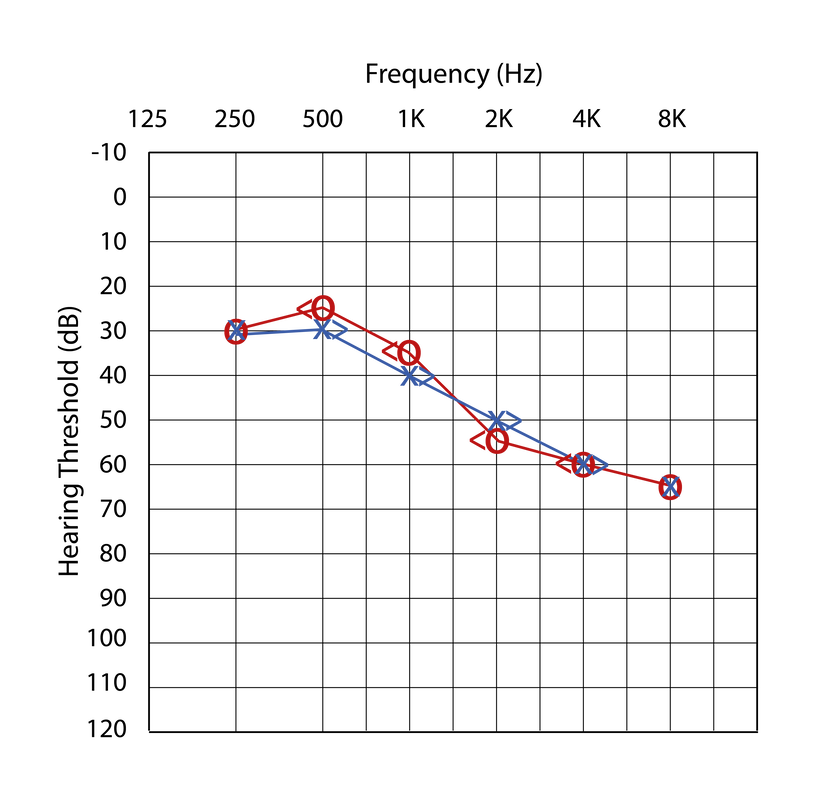
Paget’s disease is a rare and chronic bone disorder, characterized by rapid isolated bone repair. As individuals age, their bones begin to rebuild themselves at a slower rate, however, those suffering from Paget’s disease experience accelerated repair rates, often resulting in softer, abnormal bone structures. The direct cause of Paget’s disease is unknown, however, it appears to be partially due to genetics or even exposure to a particular virus. Symptoms include stiffness, numbness, constant, dull bone pain, and an elongated ear canal due to abnormal bone growth (Paget’s). Paget’s disease is commonly accompanied by sensorineural hearing loss—as seen on the audiogram—due to the abnormal growth of the skull into the nerves that connect the ears to the brain. Clinicians will typically spot Paget’s disease during an X-ray, however, blood and urine tests can also be used to determine the extent of bone involvement in their particular case. In regards to treatment, a clinician may prescribe an oral anti-inflammatory drug or even an injectable medication that can help reduce pain and aid the body in regulating the bone-rebuilding process. If managed, the disease does not seriously impact the quality of life, however, medical treatment is not expected to correct some of the changes that Paget’s disease has already caused (Monsell). Instead, clinicians aim to give the patient the best possible course of action to mediate their discomfort. |

|
TEMPORAL BONE TUMORS


|
Temporal bone tumors often manifest on the outside of the ear, especially in locations frequently exposed to the sun. They typically begin as scaly, red patches or white bumps, and may produce fluid or discharge. Genetics can play a role in the likelihood of developing such tumors, however, age, chronic sun exposure, and exposure to harmful substances such as arsenic and radiation can massively increase one’s chances (Gotter). The most common form of ear and temporal bone cancer, basal skin carcinoma, typically begins as a slow-growing bump that later becomes a painful ulcer. This particular form of temporal bone tumor can spread to the external ear canal, obstructing the normal transmission of sound and leading to conductive hearing loss, as seen on the audiogram. Other symptoms of temporal bone tumors include ear pain, discharge, and bleeding (Lobo). Many temporal bone tumors manifest in the epidermis (skin) and spread to the temporal bone portion below it, while some begin and spread from other parts of the body. Clinicians will diagnose a patient after inspecting the affected area as well as the patient’s case history. A CT scan or an MRI may be ordered to localize the growth, and if the lesion grows larger or cancer is suspected, a biopsy will be used to determine their next course of action. If cancerous, surgical removal is a more frequent treatment approach than radiation, as research shows that radiation massively increases one’s chances of sensorineural hearing loss. Some smaller tumors may be reached through the external auditory canal, while others may need access from behind the pinna (Stephanie). The temporal bone tumor has a generally positive prognosis, as long as they are caught and treated in a timely manner. |
LONGITUDINAL & TRANSVERSE FRACTURES
|
Fractures of the temporal bone are caused by head trauma and can be classified as either transversal or longitudinal, depending on the manner of the fracture. Most common, longitudinal fractures run parallel to the long axis of the petrous portion of the temporal bone and most often result from a blow to the side of the head (Patel). Such trauma can result in sensorineural and conductive hearing loss, as well as balance difficulties. Not only this, but blood in the external ear canal, facial nerve damage, and subsequent facial paralysis can also be common complications of a longitudinal fracture. Much less common, transverse fractures run perpendicular to the long axis of the petrous temporal bone and most often result from a blow to the back of the head. Facial paralysis occurs nearly 50% of the time following a transverse fracture and these fractures have the greatest risk of profound sensorineural hearing loss and severe vertigo (dizziness), as there is a disruption to the vestibulocochlear nerve (Musiek). A clinician will generally begin with a CT scan, allowing them to localize the fracture itself as well as look for possible blood in the ear canal; once they’ve done so, a more detailed temporal bone-specific CT scan can be performed. In regards to treatment, patients who have good facial nerve function following the trauma typically do well without surgery, however, without proper care, fractures have the potential to cause a host of other serious complications. If issues ensue from the temporal bone fracture, surgery may be the best course of action to prevent concerns such as stenosis (narrowing) of the ear canal, from occurring (Diaz). |


A potential audiogram depicting sensorineural hearing loss
|
