HOW IS HEARING MEASURED?
In order for a clinician to understand the type and severity of a patient’s hearing loss, they may perform a series of diagnostic tests, or, an audiological evaluation. These tests are conducted in a quiet and controlled location, typically a sound booth, using a range of octave frequencies mimicking relevant speech sounds. A clinician will use an audiometer to present the patient with signals ranging in intensities and frequencies (between 250-8000Hz). The audiometer measures responses that can be delivered using a variety of transducers, and the clinician will choose the best fit for the patient depending on their circumstances. Audiometry detects the location and the severity of the hearing loss, for example, whether it's damage to the inner, middle, or outer ear, and once the data from the test is collected, it can be plotted on a graph called an audiogram, which denotes the type, degree, and configuration of the patient’s hearing loss.
AIR CONDUCTION TESTING
|
Air conduction testing is administered by a clinician using a device called an audiometer, in which sound vibrations are transmitted to the eardrum in order to test for any obstruction of the outer, middle and inner ear. Because air conduction tests the entire auditory system, it's a frequent test used to screen a patient for hearing loss. The audiometer can transmit a wide variety of sounds at a multitude of decibels, this way, the clinician can find the patient's threshold of hearing and then better understand the type, degree, and configuration of their hearing loss. The test is administered by presenting a range of sounds with varying frequencies and intensities, the patient will then respond to the sounds that they can hear, and the clinician will decrease the volume of each tone until they can no longer hear it. Depending on the results of the test and the frequencies in which the patient could no longer hear the tones, the clinician will be able to diagnose them with one of these three types of hearing loss: sensorineural, conductive, and mixed.
|

|
BONE CONDUCTION TESTING

|
Bone conduction tests are administered when there is an obstruction of the outer or middle ear, as the sounds bypass both systems and directly tests the inner ear and the cochlea. A clinician will place a device on the patient called a bone oscillator, which is a headband with a small box that rests on the patient’s forehead or on their mastoid, a part of the skull located behind the pinna. The sounds transmitted to the inner ear will gently vibrate the bones of the skull, and the patient will respond for the sounds that they can hear by either pressing a button or raising their hand to show the clinician that they are perceiving the sounds. This test is important in helping to determine if there is a problem with the outer ear, such as the ear canal, or the middle ear, such as the eardrum or the bones of the middle ear. Once the clinician collects the results of the tests on a graph called an audiogram, they can accurately diagnose the patient with the type and severity of hearing loss.
|
READING THE RESULTS
|
When the results of air conduction and bone conduction tests are presented on an audiogram, unique symbols varying in color and shape will be used to decipher the type, degree and severity of the patients hearing loss. For both tests, red colored symbols are used to denote tests preformed on the right ear and blue symbols are used for the left ear. Sounds being transmitted during testing can also be masked, which means that another noise is played into the opposite ear being tested, preventing the intentional sounds being delivered to the patient is not crossing over to the better ear so that they can acoustically separate the testing of the two ears. In regards to unmasked air conduction testing, the symbols used to denote the patient’s response are an X and an O, which will be red if the clinician was testing the right ear and blue if they were testing the left ear. If the test is masked, in which another sound is being played in the opposite ear, the symbols used would be a Δ if the patient were being tested in the right ear and a □ if they were tested in the left ear. In regards to an unmasked bone conduction test, the symbols used to denote the patient’s response are a < when testing in the right ear and a > when testing in the left ear and for a masked test, the symbols would be a [ when testing in the right ear and a ] when testing in the left ear, all following the color descriptions that we discussed above. The configuration of the symbols as well as where they are placed on the audiogram is imperative to diagnosing the severity of the patient's hearing loss. The levels of severity—as shown on uppermost graph to the right—are dependent on where the symbols lie on the plane. The graph below it--we will discuss further in regards to the type of hearing loss that it corresponds with--models what the symbols look like once plotted on an audiogram following a test. Both ears were tested, as we can see by both blue and red symbols being used, and the sounds were unmasked, as we can tell by the X and O symbols being used.
|


|
CONFIGURATIONS
During an audiological evaluation, the results plotted on an audiogram will have varying configurations depending on the frequencies in which the patient could best hear the tone. Difficulty hearing sounds with high frequencies is called “high frequency loss” while difficulty hearing low frequencies is “low frequency loss." The figure to the left depicts six possible configurations that may be presented during an audiogram, and as we know, the y-axis represents the patient's hearing level in decibels and the x-axis represents the frequency of the tone being played in hertz.

|
A flat configuration would be representative of a patient with hearing abilities more or less the same at all frequencies, and is depicted as a straight horizontal line on the audiogram.
A rising configuration indicates that high-frequency sounds can be heard better than low-frequency sounds. A sloping configuration indicates that there is little to no hearing loss at low frequencies. A precipitous hearing loss indicates mild hearing loss in the lower frequencies, and much worse for the higher frequencies. A notch configuration depicts a noise-induced hearing loss, with a sharp decrease in hearing level. A corner configuration indicates severe hearing loss, with the patient only being able to hear very little at low frequencies. |
TYPES OF HEARING LOSS
Hearing loss can be both bilateral, meaning that there is hearing impairment in both ears, or unilateral, where hearing loss only present in one ear. Not only this, but hearing loss results on an audiogram can depict both symmetrical and asymmetrical configurations. Symmetrical hearing loss means that the severity and the shape of the hearing loss is very similar in both ears, this may be due to repeated exposure to noise damaging equipment, effecting the impairment in both ears. Asymmetrical hearing loss occurs when the shape and severity of impairment is not the same in both ears, which is more common in geriatric patients or those who have been exposed to damage in a particular ear. In regards to the type of hearing loss, patients can experience sensorineural, conductive, or mixed hearing loss. The type of hearing loss present is dependent on where in the auditory system that the impairment occurs.
|
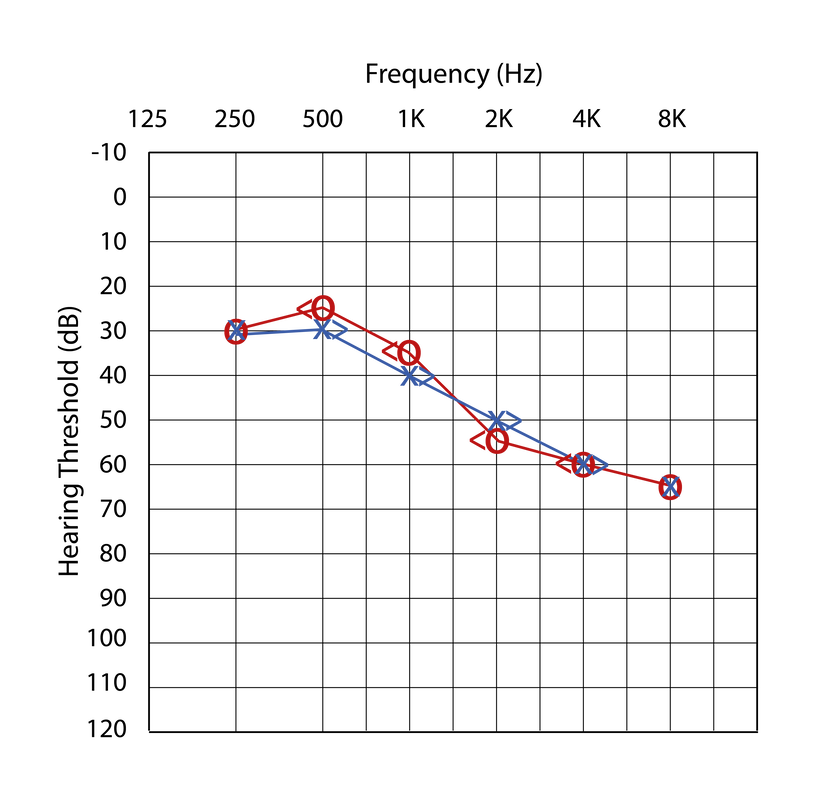
Sensorineural hearing loss is characterized by impaired bone conduction and air conduction tests, with the thresholds being within ten decibels of each other, as seen in the audiogram to the right. It's signified by impairment in the inner ear, meaning that there is no loss in the conduction of sound. |
|
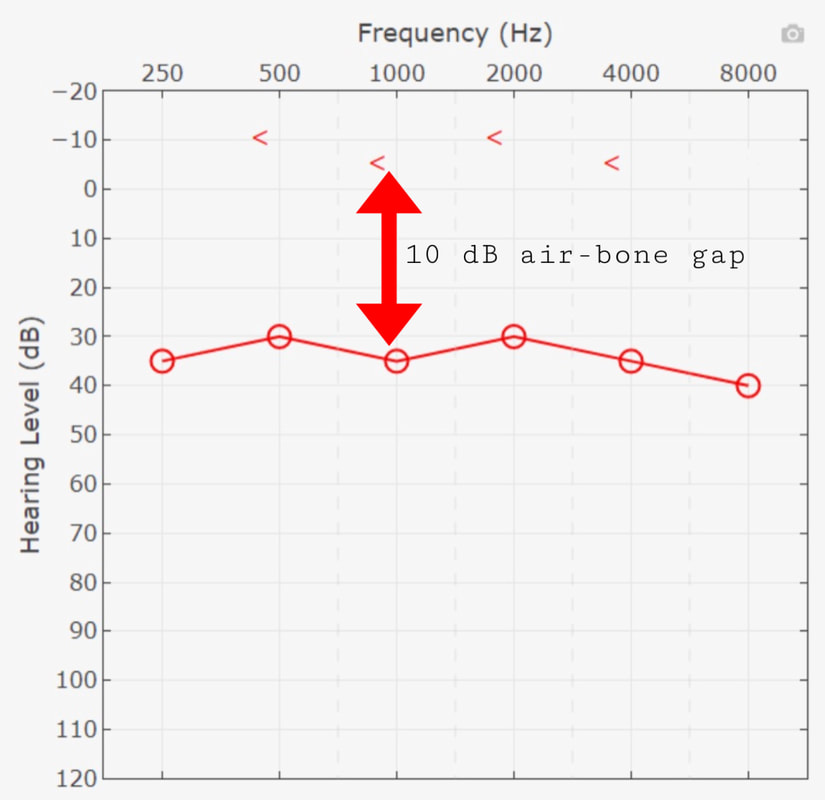
Conductive hearing loss is characterized by a normal bone conduction test and an impaired air conduction test, meaning that there is loss in the conduction of sound, or, some kind of obstruction of the outer or middle ear. There is no impairment in the inner ear, or the cochlea and beyond, as the bone conduction results were normal. Another key feature to conductive hearing loss is that of an air-bone gap, meaning that there is a ten decibel or greater difference between the frequency thresholds of the air conduction test and the bone conduction test. |
|

|
Mixed hearing loss is characterized by impaired bone conduction and air conduction tests, and the air conduction results are typically worse. There is also a presence of an air-bone gap, and hearing loss is often visible across all frequencies |
SPEECH TESTS
Speech tests may be administered to demonstrate a patient's potential loss of word recognition ability, or even to determine whether or not they are in need of a hearing aid device. Not only this, but the tests can detect whether or not an individual's device is working properly, and if it needs to be altered to best suit their need for amplification. One's Speech Recognition Threshold (SRT) is denoted as the softest level in which an individual can understand 50% of a list of two-syllable words. Measured in dBHL (decibels hearing level), it asks, what is lowest dB that the individual can hear the words? Puretone Average (PTA) refers to the average of hearing threshold levels at a set of specified frequencies: typically 500, 1000, and 2000 Hz. Once the results of an audiogram are plotted on the graph, the hearing levels (dB) found at these three frequencies are averaged in order to get an idea of the individual’s hearing levels in each ear and whether or not they are within normal limits. If that is the case, their SRT score should be within seven to ten decibels of their PTA score.
|
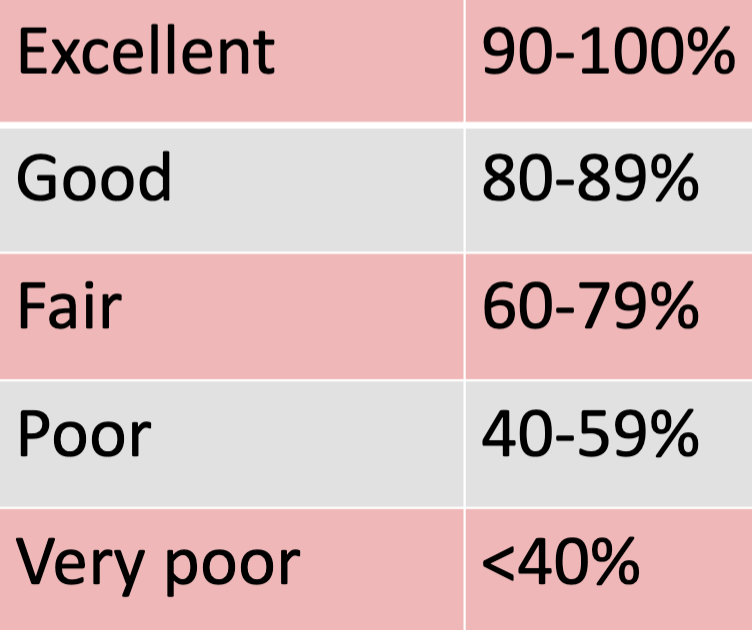
Word Recognition Ability (WRA) is a test used to detect the optimum performance for word recognition of a closed-set list of words, resulting in a Word Recognition Score (WRS) recorded as a percentage, as seen to the right. The test reflects the ability of a patient to discern between twenty-five different words delivered at their patient’s MCL, or most comfortable level, which is where the speech is most clearly heard (Venema). Depending on how well the patient is able to repeat the words back to the clinician, will determine their word recognition score, which is scaled on a chart like the one depicted here.
|
|

Speech in Noise Test (SIN) is an evaluation of how well a patient is able to discern speech in an environment with background noise. It's a more realistic testing scenario, as it mimics real world situations, and the sounds progressively get louder as the test goes on. The test can be used to asses the functional capacity of the individual and for clinical diagnoses, as it gives the clinician a better idea of the patient's real-world hearing abilities (Portnuff). Both parties benefit greatly from the nature of a SIN test, as the clinician has a better ida of how to provide the patient with the adequate resources to improve their hearing.
